 Yes
Yes  No
No
 Yes*
Yes*  No
No Yes
Yes 
 No
NoWe were developing this PDF editor with the idea of allowing it to be as effortless make use of as possible. This is why the actual procedure of creating the ancc education validation form will likely to be easy as you go through all of these steps:
Step 1: The first task will be to pick the orange "Get Form Now" button.
Step 2: Right now, you can begin modifying the ancc education validation form. Our multifunctional toolbar is at your disposal - add, eliminate, modify, highlight, and undertake other commands with the content material in the form.
Type in the details demanded by the application to prepare the document.
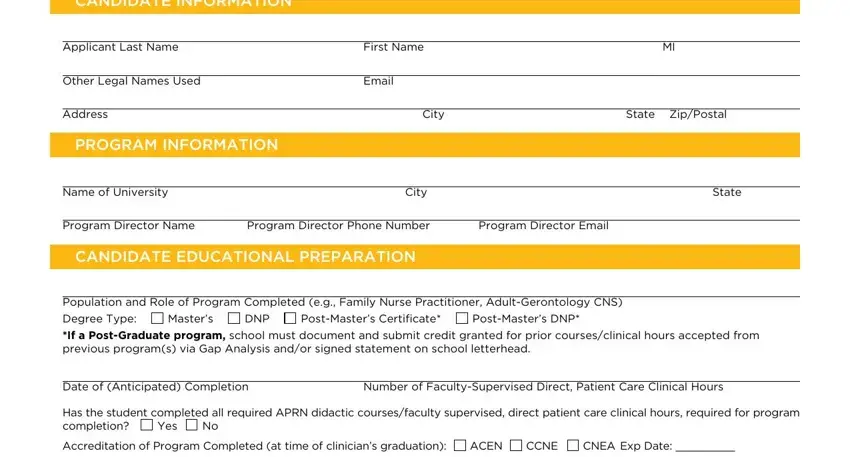
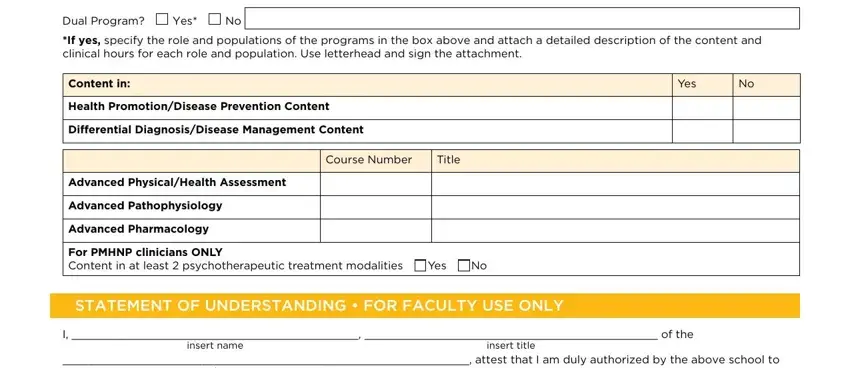
Jot down the details in Dual Program, Yes, If yes specify the role and, Content in, Health PromotionDisease Prevention, Differential DiagnosisDisease, Course Number, Title, Advanced PhysicalHealth Assessment, Advanced Pathophysiology, Advanced Pharmacology, For PMHNP clinicians ONLY Content, Yes, STATEMENT OF UNDERSTANDING FOR, and I of the.
You're going to be instructed to write down the details to let the program complete the segment Forms received without a signature, Required Program Director Signature, Print Name, Date, ANCC reserves the right to request, and CPMFRM Validation of APRN.

Step 3: Hit "Done". Now you can upload your PDF file.
Step 4: It's going to be more convenient to have copies of the file. There is no doubt that we are not going to share or view your information.
